Intro to EKG Interpretation - Myocardial Infarctions (Part 1 of 2)

Vložit
- čas přidán 1. 07. 2014
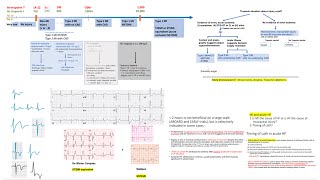
- A review of the EKG findings in MIs, including their morphological classification, a determination of their age, and localization to region of the heart and likely culprit vessel.








Thanks Dr Eric Strong . I understand this now. from cannot read anything in EKG to be able to read some. Huge progress. I own you a debt of gratitude.
Thanks a lot man.
I have my MIR ( Spanish Pre- Residence test next week).
We usually get 2 to 4 EKGs and they were a couple things neither books, classes or other videos had been able to clarify to me. The fact that you take the time to explain the reason why things happen makes it eassy to memorize and use later.
Of you are ever considering another topic. You should considering adding ion channel diseases. We often get EKGs of Brugada Disease as so Rome Warg has been asked. And Type II.
They also like to add Tako Ando. Right Arrithmogenic and Hypertrophic specially the apex one. ( Yes they expect us to be encyclopedias with legs is not very usual to expect that a last year Med student knows those things).
Last year they had an EKG of a pathient with vascular endothelial dysfunction and 98% of the testers failed it. ( They add this crazy questions because they rank us 14.000 of us and it helps to stratificate).
At any case I will recomend your videos to a couple friends they are awesome.
Wow- seriously makes me think about just taking online classes because I completely understood everything.
thank you very much for the excellent lectures Really
appreciate your time and very clear presentations on several complex
topics
Dear Eric Strong, very thank you for ECG interpretation and explanation. They help me to theach my students. Sorry for my poor english.
Thank Dr Eric. You've helped me a lot.
A high quality lecture. It helps me more to understand MI..... Excellent!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! (y)
A life saving video .. Thank you for the great explanation..
U know what... ur amazing.
Hello Eric, thanks for the excellent video this is very helpful, but I still find it very difficult to tell if there is a pathological Q wave. I have looked up the criteria for it but do not find it very helpful, and find it hard to find specific examples of pathological q waves. Could you do a video to help clear this up like your other videos do? :)
From goldberger’s : “normal septal q waves must be differenti- ated from the pathologic Q waves of infarction. Normal septal q waves are characteristically nar- row and of low amplitude. As a rule, septal q waves
are less than 0.04 sec in duration. A Q wave is gen- erally abnormal if its duration is 0.04 sec or more in lead I, all three inferior leads (II, III, aVF), or leads V3 to V6.
What if Q waves with duration of 0.04 sec or more are seen in leads V1 and V2? A large QS com- plex can be a normal variant in lead V1 and rarely in leads V1 and V2. However, QS waves in these leads may be the only evidence of an anterior septal MI. An abnormal QS complex resulting from infarc- tion sometimes shows a notch as it descends, or it may be slurred instead of descending and rising abruptly (see Fig. 8-9). Further criteria for differen- tiating normal from abnormal Q waves in these leads lie beyond the scope of this book.”
Thank you so much sir
Seen jst nw wat u made 6 yr back
It's amazing...do more & more videos sir
This was amazing. Thank you!
Awesome video! I was wondering whether reciprocal change is an acute phenomena...so not seeing reciprocal change in the inferior leads (in the seeing of ST elevation in V3-V4) also tips you off that you may not be dealing with an acute MI as in your second example??? However the large Q and T wave inversions do give it away.
Nice video Doc. Good information.
Thanks soo much.. I have been struggling to understand ECG
You are excellent teacher
Excellent video, thank you very much
I have heard of a way to more easily diagnose a right ventricular MI than looking close at V1 and V2 for a right ventricular pattern. That is to put the precordial leads on the right side of the chest. I have heard of these right ventricular leads being referred to as V7-V12.
Dr strong, thank you from singapore :)
I like this video really is very important for my understanding
Interpreting like a boss!
Thank you Dr Strong
Good afternoon...
I have a doubt in the ekg of example 3,
You are saying inferior wall got affected ,because of Q wave , but there is no prominent q wave in lead2, okay we can consider it as inferior wall bcs other two leads are having prominent q wave ....
Amidst of this, i have seen ST elevation in v1 and v2 , why can't we conclude this as posterior or septal wall? And in example 4, there is ST elevation in v2,v3,v4 too..
I couldn't understand this
Please can you shed some light on it?
Outstanding!
Thank you so much sir the best explanation
Hello Eric Sir... i am a huge fan of your videos... just wanted to ask... in EKG at 15:50 time there are ST depressions in lateral leads... are they significant or not... it appears that this infarct is not really that old... can u give ur expert opinion?
Thanking you in anticipation
Hey Dr eric .. you seem like a very successful doctor .. Do you mind sharing what books you read for motivation ?
I generally don't read motivational-type books. During the rare moments when I have time for reading, it's usually literary fiction or "pop physics" (e.g. Brian Greene), although right now I'm reading "Ending Medical Reversal" by Vinay Prasad and Adam Cifu (which is almost anti-motivational, since it discusses all of the mistakes the medical profession has made in recent decades, and some which we are continuing to make!)
@@StrongMed ولك لاااااااااااااا مش هيك يهبل
Wonderful video🎉❤
Nice work.....تم
PERFECT!
Looking at example 1, does the distal PDA ever occlude causing inferior infarction/changes but no posterior infarction/changes? If it can occur would that look similar or different to this example?
Well, there are a couple of notes I'd like to adress here Dr, if I may. First, although I absolutely agree with the fact that it is incorrect to claim STEMI = QwaveMI and NSTEMI = Non QWave MI, I find it also incorrect to vastly claim that NSTEMI (St depressions) or Qwaves dont show the area where the lesion is present. Take ECG numer 3 for instance, yes, we just had a Qwave in II (barely) III and AVF, but, as you mentioned, reciprocal changes are important. And there is a r wave in V1, which within the context of a probable inferior old MI, would support the logic that the patient had, as a fact, a Postero-Inferior MI, thus the r wave in V1 could be actually projecting a Q wave from the posterior area of the heart, and if we focus on the Amplitud of this r wave in V1, it shares voltage with the q wave in II. Therefore, I do consider is extremely important to be careful when we give specific qualities to certain interpretations in the ECG, and the claim Q waves or ST depressions will not show the affected territory, in my opinion, is just wrong. Also, you mentioned an ST depression in the context of a NSTEMI could lead to a Qwave, well, I'd be happy to hear an explanation on how. Q waves are in short terms "windows" of the electrical activity being read in the opposite side of the actual lead, because we do not have electrical depolarization in that area (a scar has formed, and conective tissue is not a good electric conductor) therefore what we read with the electrode will be the vector pointing out in the opposite direction (because the opposite side of the heart musscle is in fact conducting electricity), and because a ST depression what is actually showing is a subendocardic ischemic area, in the context of a NSTEMI that has not progressed to a full MI because of medical intervention for example, there is no electrophysiological reason to expect it to present as a Q wave later on.
That being said, I thank you deeply for sharing this content, it's always positive to see how ECG interpretation is being explained.
Greetings and best regards Dr.
How does one identify pathologic q wave in leads V1-V3? Aren't these predominantly supposed to be negative deflections in these leads anyways?
Thank you so much! 2/8/2019 😁
U comments in every video related to ECG 😁
AWESOME DISCUSSION
Dear Dr. Strong,
What exactly is the (clinical (?)) relevance for the high lateral leads (i.e. why should one do this distinction)?
Thank you very much in advance for your answer.
Kind regards,
many thanks
As in Example 3, I see the Qs in 11 and aVF but not in lead 111. Why you said that the EKG strongly suggest LVH as the cause rather ischemia/infarction. According to my EKG book by K Ellis, 4th edition, the most commonly used criteria of LVH is R wave in V5 or V6 ( whichever is taller) + the S wave in V1 or V2 is greater than or equal 35mm. I don't see that criteria as LVH. Could you explain why the cause is LVH rather than infarction/ischemia? I see ST elevation in V1 and V2. There is a probability of LBBB instead of LVH. What do you think Doc?
There are "physiological septal" Q waves in the lateral leads (V5, V6. I, and aVL), which would have been absent if the left bundle branch of Tawara was blocked (the normal septal depolarisation is stemming from that bundle).
Regarding the left ventricular hypertrophy (LVH), there are multiple criteria and some of them, such as the Cornell, Lewis, and Romhilt-Estes are actually consistent with LVH in this specific example on 16:00
Thank you so much
Thanks doc with your asisst
Its great❤
very Good!!!
Eric mentioned that example 3 contains a pathological Q wave in leads II, III and aVF. Can someone confirm/refute this in lead II? Either I'm not seeing it or I don't understand what pathological Q waves are. I do see Q waves in leads III and aVF.
Also, Eric said that there are no ST elevations in example 3 but I think I'm seeing ST elevations in leads V1 and V2 (though I do understand that ST elevations can occur in these leads as a normal variant).
Heikki Salmenperä You are absolutely correct. I think I got a little lazy with my narration for that example. There are pathological Q waves in III and aVF; the tiny q in II shouldn't count as pathological. And there are ST elevations in V1 and V2, though both their specific morphology (concave upwards and upsloping into an upright T wave) and context of the entire EKG strongly suggest they are from LVH rather than ischemia. (I'll place an annotation to clarify).
Eric's Medical Lectures Thank you for the rapid clarification!
Pathologic Q waves are a sign of previous myocardial infarction.
Great sir
god bless you DR
ahlam majali a see a
Thank you sir
Gr8 one thanx
excellent
excellente
In example 4, the q wave is not that deep in lateral leads, besides the ST elevation and positive T in the same leads. Doesn't this make it an acute lateral MI, in addition to the already mentioned subacute inferior MI?
in example 2, are there pathological Q waves in v1 as well?
Any intention to make a video about OMI, NOMI , MINOCA ? Every now and then I watch some of your videos. Thanks !!
Thanks for the suggestion! Yes, the Meyers-Weingart-Smith OMI paradigm is a planned future video in the EKG series. Just haven't gotten to it yet - unfortunately, too many other requests/needs!
Would you say Example 1 is actually an acute inferior-posterior STEMI?
In example 3, what are the changes in V2?
You rock
Can't see any Q waves what am I looking for?
In example 2, why is there no reciprocal changes ?
Sometimes acute STEMIs just don't have reciprocal changes visible on the EKG. Sorry I don't know of a better explanation. ¯\_(ツ)_/¯
how can I have online classes
Sir please make videos on EEG interpretation
I'm very sorry, but I only make videos on topics related to my own clinical experience. EEG interpretation is too far outside my scope of practice.
تم التحميل....
😔 why can’t you circle the areas in the examples :(
What is yours books
voice too soft, not catching many words