STEMI part 1: focus on reperfusion- Elias Hanna

Vložit
- čas přidán 26. 07. 2024
- **Ideas of this talk are from chapter 2 of my book, Practical Cardiovascular Medicine, Wiley 2022
0:00 Timelines: physiology and streamlined management (inspired by guidelines)
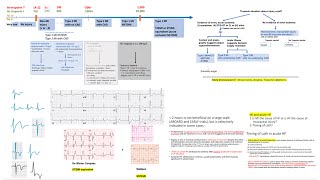
12:21 Brief on management beyond 24 hours and OAT trial, and ECG features of late STEMI
22:33 Brief on ECG features and on new LBBB
26:50 When to give fibrinolytics in transfer patients: equipoise door-to-balloon time, importance of ischemic time (more or less than 3 hrs), risk profile, age over 75. Trials and efficacy curve of PCI vs fibrinolysis (31:57)
39:16 When to do PCI after fibrinolysis: rescue PCI, pharmacoinvasive PCI. Definition of response to fibrinolytics (40:20)
44:35 and 34:20 Bottom line approach for transfer patients
47:10 Fibrinolytics pharmacology (47:10), efficacy (06:42), adjunct therapy (50:37), contraindications (36:32), how to define response (40:20), and doses (59:12)
59:12 r-tpa dose: 15-50-35 (not 30): 15 mg bolus-then 50 mg over 30 min-then 35 mg over 60 min (total 100 mg). Weight adjust the dose in patients less than 67 kg
52:01 Case illustrations/ECGs/management
1:00:25 Case of transient ST elevation
1:03:40 Case of a responder to fibrinolytics, how to manage over 24 hrs later
1:08:12 Multivessel CAD and non-culprit PCI. Define what is significant non-culprit stenosis. Cases of shock and STEMI, shock and NSTEMI
1:14:06 CABG for multivessel CAD after STEMI








Fascinating as always
thank you for explained so clearly, cant wait for part 2 thanks
Fascinating lecture as usual
Absolutely fantastic
Very Great Work , Thanks deeply
Thanks greatly!
many thanks for Ur magnificent videos and valuable book really waiting for more videos
Fantastic ❤❤❤ thank you so much
Thank for your book best ever
Very Informative and comprehensive. Dr Elias Hanna can you please give a lecture/ lectures on how to perform primary PCI. Thanks
thank u very much 💚💚💚
Great video as always
Can you make a video on Access and Closure devices? Would be very useful for general fellows
Very detailed presentation thank you. What are your views about Enhanced External Counter Pulsation therapy post procedure period or prior to angioplasty in patients who are electively posted for angioplasty
still confusing on factor arguing against lytic
what is lower risk STEMI?
Post stemi id mild pain present 2/3 out of 10 but describes the exact same quality of pain just milder…how you interpret this? As some suggest any same pain regardless of mild is pain.
I mentioned that after STEMI, including after STEMI reperfusion, the patient frequently has mild bruising pain 1-2/10. The key is that this pain is perceived as much milder by the patient, and he is not in distress (he wants to eat and chat, no nausea, no diaphoresis,...).Take into account the degree of distress the patient appears to be in, and how much better this pain is compared to the initial pain. If he appears uncomfortable, this is true STEMI pain.
Also, like I explain in this talk and more so in STEMI part 2, I use 3 features to decide late presentation (no ongoing STEMI pain, >24 hrs timeline, and ECG pattern of very deep Q with relatively mild residual R and ST elevation). If all 3 are present, it is late; if 2 of 3 are present, it is likely late. So look at the full picture.
Since there is subjectivity in all those features, IN CASE OF ANY DOUBT, cath the patient emergently. Recanalizing an occluded artery later than 24-48 hrs is not beneficial per OAT, but not particularly harmful either; so recanalize it in case of doubt.
Quick question sir, how do you manage anticoagulation in those who you give lytics to ?
Along with lytics and as they are getting transferred, we give aspirin 325 mg, clopidogrel 300 mg (75 mg if older than 75, but we complete it to 300 mg when they undergo PCI)
+UFH IV bolus 60 units/kg (not more than 4000 units), followed by heparin drip 12 units/kg/h along with lytics.
As long as PCI is planned within the next 24 hrs, which should be the standard care, we don't use enoxaparin. Enoxaparin IV bolus followed 15 min later by SQ dose used to be a good and rather preferred strategy in patients treated purely with lytics without plans for PCI in the first 24 hrs (EXTRACT TIMI trial), but this is not the standard in the pharmacoinvasive era and trials.
@@eliashanna8248 Thank you for the elaborate answer. Given the result of TREAT trial, the high thrombotic nature of STEMI, do you ever use ticagrelor in STEMI patients who had been given lytics?
I think as explained in video, ticagrelor and parasugrel should not be used
@@namphan6911 Great point regarding TREAT trial. Previously, PLATO trial of ticagrelor excluded pts within 24 hrs of lytics and this is what drove the guidelines. TREAT randomized patients who already received lytics and mostly already received clopidogrel 300 mg load to ticagrelor (vs continuing clopidogrel) within 24 hrs of lytics. IT showed ticagrelor is safe and feasible from a bleeding standpoint. Note that ~50% of those pts eventually underwent PCI
Sir, congrtz for your chanell